Hey SOCMOBBERS,
I have a new video on how to make your own end-tidal CO2 detector for a face mask or non-rebreather. Check it out here.
Cheers,
Chris
@SOCMOBEM
Wednesday, 13 March 2013
Friday, 8 March 2013
SOCMOB has moved!
Hi all,
SOCMOB has moved to Wordpress. Go to www.socmob.org to check out the new site, sign up for RSS feeds, tweets, etc.
All new content will now be appearing there.
Thanks for reading,
SOCMOBEM
SOCMOB has moved to Wordpress. Go to www.socmob.org to check out the new site, sign up for RSS feeds, tweets, etc.
All new content will now be appearing there.
Thanks for reading,
SOCMOBEM
Wednesday, 27 February 2013
NSAIDs part 2: The Ceiling Effect
Sorry readers. I've been slacking off on vacation in NYC, eating too much and blogging about food more than medicine. Tonight at dinner with Mr. EMCrit, Scott called me out a bit for insufficient content. Also, one of my readers has some rounds coming up soon, and needs to talk NSAIDs. With that in mind, here's part 2 of the NSAID saga.
In part 1 on NSAIDs, we looked at NSAID equivalency for analgesia and the myth that is ketorolac (Toradol).
Hat tip to readers Moshe and Elisha (@ETtube on twitter) for pointing out the concept of the ceiling effect with NSAIDs. I did not mention this in part 1, and will discuss it today.
There's a great talk by Larry Raney on the Free Emergency Talks website that discusses NSAIDs and the ceiling effect. You can find it here. As an aside, the Free Emergency Talks website is run by Joe Lex, one of the great EM educators, and has a thousands of talks from any conference you can think of.
What is the ceiling effect?
 * Free sammich to the first reader who tells me where this ceiling is. (Sammich will be good when it goes in the mail, but I can't guarantee quality on arrival. Might make it a cockroach and twinkie sammich to prevent spoilage.)
* Free sammich to the first reader who tells me where this ceiling is. (Sammich will be good when it goes in the mail, but I can't guarantee quality on arrival. Might make it a cockroach and twinkie sammich to prevent spoilage.)
The ceiling effect is the concept that there is a maximum level of analgesia that can be reached with a dose of medication, and beyond that dose, you get no more analgesia.
In addition, you continue to get more side effects. That double sucks!
Tylenol and NSAIDs classically fall into the category of analgesics with a ceiling, while opiates have no ceiling. This is why we can bomb in loads of fentanyl or morphine, but you don't see us pounding patients with ibuprofen.
If you look at the doses of NSAIDs listed in part 1, you'll see some pretty whopping doses.
Aside from the ceiling of anti-inflammatory dosing, there is also the concept of a second ceiling for acute pain?
Two ceilings? Yup, two ceilings.
The ceiling dose for acute pain with ibuprofen is 400 mg po.
The higher ibuprofen dose ceiling of 800 mg I mentioned in part 1 is the anti-inflammatory ceiling of the NSAID and comes from the rheumatology literature. I apologize if I confused anyone with this. One key to understanding the NSAID literature is that it generally comes from 3 patient groups: rheumatologic disease, post-operative pain and dental pain. The latter two are probably both representative of pain we see in ED patients, ie: acute, non-inflammatory pain.
This is the reason why meta-analyses of NSAID efficacy are a challenge; the indications, duration of therapy, dose, etc. are completely different. In some studies, you are looking at patients with chronic inflammatory conditions on long term therapy. These patients may need higher dose NSAIDs for their anti-inflammatory effects. In other studies, it is single dose or short-term NSAIDs where analgesic ceiling will be 400 mg.
You can see how lumping all of these studies together in a review would misconstrue pretty much any endpoint.
Let's now look at the two main studies supporting the 400 mg ceiling dose of ibuprofen and 10 mg ceiling dose of ketorolac.
In contrast to the usual scenario in which old research = bad research (or a HSSP: High School Science Project), there are papers from 1978 and 1986 looking at the ibuprofen ceiling effect.
The first, by Winter et al. in 1978 looked at 510 post oral surgery patients who had 1 or more extractions, impactions and even a few with alveolectomies. That all sounds pretty painful! They compared five treatments: ibuprofen 400 mg, ibuprofen 800 mg, ASA 650 mg, Darvon 65 mg and placebo. Both ibuprofen groups had similar reduction in pain scores and were better than the other 3 treatment arms. The study was done with pooled data from two separate dentists; in one group 400 mg ibuprofen seemed slightly more effective, while 800 mg seemed slightly more effective in the other. However, there are no data to support any statistically significant difference between ibuprofen groups in the article.
The second article, by Laska et al. in 1986 was a double blind parallel group study with 200 patients post oral surgery compared doses of 400 mg , 600 mg and 800 mg of ibuprofen. There was no evidence of a dose response efficacy difference between 400, 600 and 800 mg.
Considering that dental pain hurts like hell, I'm inclined to believe these studies are sufficiently representative of ED patients with most injuries. *As an aside, learn to do dental blocks, they are invaluable to patients.
With regards to ketorolac, this double blind RCT from Staquet in 1989 compared 10 mg, 30 mg and 90 mg IM ketorolac with placebo in 128 patients with cancer pain. Again, no difference was found between the 3 ketorolac dosing regimens, with all being much superior to placebo.
Other similar studies have been done and show 10 mg is probably the ceiling dose of ketorolac both orally and parenterally.
In the next parts of the NSAID saga, we'll discuss side effects profiles of various NSAIDs, and NSAID hodgepodge such as effect on fracture healing, use in renal colic and more.
Cheers,
SOCMOBEM
References:
Winter et al. Oral Surg Oral Med Oral Pathol. 1978 Feb;45(2):159-66.
Laska et al. Clin Pharmacol Ther. 1986 Jul;40(1):1-7.
Staquet MJ J Clin Pharmacol. 1989 Nov;29(11):1031-6.
In part 1 on NSAIDs, we looked at NSAID equivalency for analgesia and the myth that is ketorolac (Toradol).
Hat tip to readers Moshe and Elisha (@ETtube on twitter) for pointing out the concept of the ceiling effect with NSAIDs. I did not mention this in part 1, and will discuss it today.
There's a great talk by Larry Raney on the Free Emergency Talks website that discusses NSAIDs and the ceiling effect. You can find it here. As an aside, the Free Emergency Talks website is run by Joe Lex, one of the great EM educators, and has a thousands of talks from any conference you can think of.
What is the ceiling effect?
The ceiling effect is the concept that there is a maximum level of analgesia that can be reached with a dose of medication, and beyond that dose, you get no more analgesia.
In addition, you continue to get more side effects. That double sucks!
Tylenol and NSAIDs classically fall into the category of analgesics with a ceiling, while opiates have no ceiling. This is why we can bomb in loads of fentanyl or morphine, but you don't see us pounding patients with ibuprofen.
If you look at the doses of NSAIDs listed in part 1, you'll see some pretty whopping doses.
Aside from the ceiling of anti-inflammatory dosing, there is also the concept of a second ceiling for acute pain?
Two ceilings? Yup, two ceilings.
The ceiling dose for acute pain with ibuprofen is 400 mg po.
The higher ibuprofen dose ceiling of 800 mg I mentioned in part 1 is the anti-inflammatory ceiling of the NSAID and comes from the rheumatology literature. I apologize if I confused anyone with this. One key to understanding the NSAID literature is that it generally comes from 3 patient groups: rheumatologic disease, post-operative pain and dental pain. The latter two are probably both representative of pain we see in ED patients, ie: acute, non-inflammatory pain.
This is the reason why meta-analyses of NSAID efficacy are a challenge; the indications, duration of therapy, dose, etc. are completely different. In some studies, you are looking at patients with chronic inflammatory conditions on long term therapy. These patients may need higher dose NSAIDs for their anti-inflammatory effects. In other studies, it is single dose or short-term NSAIDs where analgesic ceiling will be 400 mg.
You can see how lumping all of these studies together in a review would misconstrue pretty much any endpoint.
Let's now look at the two main studies supporting the 400 mg ceiling dose of ibuprofen and 10 mg ceiling dose of ketorolac.
In contrast to the usual scenario in which old research = bad research (or a HSSP: High School Science Project), there are papers from 1978 and 1986 looking at the ibuprofen ceiling effect.
The first, by Winter et al. in 1978 looked at 510 post oral surgery patients who had 1 or more extractions, impactions and even a few with alveolectomies. That all sounds pretty painful! They compared five treatments: ibuprofen 400 mg, ibuprofen 800 mg, ASA 650 mg, Darvon 65 mg and placebo. Both ibuprofen groups had similar reduction in pain scores and were better than the other 3 treatment arms. The study was done with pooled data from two separate dentists; in one group 400 mg ibuprofen seemed slightly more effective, while 800 mg seemed slightly more effective in the other. However, there are no data to support any statistically significant difference between ibuprofen groups in the article.
The second article, by Laska et al. in 1986 was a double blind parallel group study with 200 patients post oral surgery compared doses of 400 mg , 600 mg and 800 mg of ibuprofen. There was no evidence of a dose response efficacy difference between 400, 600 and 800 mg.
Considering that dental pain hurts like hell, I'm inclined to believe these studies are sufficiently representative of ED patients with most injuries. *As an aside, learn to do dental blocks, they are invaluable to patients.
With regards to ketorolac, this double blind RCT from Staquet in 1989 compared 10 mg, 30 mg and 90 mg IM ketorolac with placebo in 128 patients with cancer pain. Again, no difference was found between the 3 ketorolac dosing regimens, with all being much superior to placebo.
Other similar studies have been done and show 10 mg is probably the ceiling dose of ketorolac both orally and parenterally.
In the next parts of the NSAID saga, we'll discuss side effects profiles of various NSAIDs, and NSAID hodgepodge such as effect on fracture healing, use in renal colic and more.
Cheers,
SOCMOBEM
References:
Winter et al. Oral Surg Oral Med Oral Pathol. 1978 Feb;45(2):159-66.
Laska et al. Clin Pharmacol Ther. 1986 Jul;40(1):1-7.
Staquet MJ J Clin Pharmacol. 1989 Nov;29(11):1031-6.
Thursday, 14 February 2013
Battle Preparation 2: The Buddy Shift
This is the 2nd part in the Battle Preparation series by SOCMOB guest blogger Damon Tedford.
In part 1, we looked at a checklist of items that new learners and staff should identify and examine prior to their first shift in a new ED. Today we will be looking at the critical questions to ask on your buddy shifts before venturing off alone in your new ED. These posts are most oriented to the level of senior residents who will become new staff physicians in the near future. However, the checklists will also be very beneficial to anyone entering a new department, including nurses, junior residents, respiratory therapists, etc. The ability to find proper equipment is more important than the proper strategy in dealing with a problem. Amateurs discuss strategy, experts discuss logistics.
Important questions in this document include:
- What radiology tests do I have access to, and at what times of day?
- How do I set a patient up for outpatient antibiotic therapy?
- Is there a crisis worker for psychiatric patients or do I see them first?
- What are the expectations in our group for shift handover?
and many more...
Let me use a story to emphasize the importance of logistics versus strategy. A few months ago on a CCU rotation, I was managing a chest pain patient in the ED. He had hyperacute T-waves on his ECG. It was about 2 AM, the ED was packed, and it would be about 45 minutes until he could get to the cath lab. In the meantime, he required management of his chest pain and a nitroglycerin infusion had been started at 10 mcg/min. His nurse was only intermittently in the room, so frequent titration of his nitro would have been impossible unless I knew how to do it myself. Fortunately, I had made sure to learn to use our IV pumps; thus I could quickly increase his nitro infusion independent of nursing staff requirements.
This same concept applies to everything you do in the ER; from inserting a urinary catheter to preparing a patient for inter-department transport. Self-reliance and total logistic knowledge of your environment is a must. Pretend you're an anesthetist. Have you ever seen an anesthetist who didn't set up his/her own pumps or draw up his/her own meds?
Here is a link to part 2 of the Battle Preparation: Buddy Shift Questions
Cheers,
Damon Tedford (@DamonTedford), Chris Krause and Chris Bond (@SocmobEM)
In part 1, we looked at a checklist of items that new learners and staff should identify and examine prior to their first shift in a new ED. Today we will be looking at the critical questions to ask on your buddy shifts before venturing off alone in your new ED. These posts are most oriented to the level of senior residents who will become new staff physicians in the near future. However, the checklists will also be very beneficial to anyone entering a new department, including nurses, junior residents, respiratory therapists, etc. The ability to find proper equipment is more important than the proper strategy in dealing with a problem. Amateurs discuss strategy, experts discuss logistics.
Important questions in this document include:
- What radiology tests do I have access to, and at what times of day?
- How do I set a patient up for outpatient antibiotic therapy?
- Is there a crisis worker for psychiatric patients or do I see them first?
- What are the expectations in our group for shift handover?
and many more...
Let me use a story to emphasize the importance of logistics versus strategy. A few months ago on a CCU rotation, I was managing a chest pain patient in the ED. He had hyperacute T-waves on his ECG. It was about 2 AM, the ED was packed, and it would be about 45 minutes until he could get to the cath lab. In the meantime, he required management of his chest pain and a nitroglycerin infusion had been started at 10 mcg/min. His nurse was only intermittently in the room, so frequent titration of his nitro would have been impossible unless I knew how to do it myself. Fortunately, I had made sure to learn to use our IV pumps; thus I could quickly increase his nitro infusion independent of nursing staff requirements.
This same concept applies to everything you do in the ER; from inserting a urinary catheter to preparing a patient for inter-department transport. Self-reliance and total logistic knowledge of your environment is a must. Pretend you're an anesthetist. Have you ever seen an anesthetist who didn't set up his/her own pumps or draw up his/her own meds?
Here is a link to part 2 of the Battle Preparation: Buddy Shift Questions
Cheers,
Damon Tedford (@DamonTedford), Chris Krause and Chris Bond (@SocmobEM)
Saturday, 9 February 2013
NSAIDs Part 1: Which one is best?

I
love NSAIDs! Yup, love ‘em!
NSAIDs
(Non-steroidal anti-inflammatory drugs)
are some of the best analgesics available, plus they’re generally over the
counter. Despite their daily use for decades, NSAIDs remain sorely misunderstood. I know they’re not a
panacea, and they have some serious side effects in certain
populations. But for healthy patients without co-morbidities, they
are pretty awesome painkillers, with no addictive potential (that I’m aware
of).
Before we start,
perform a Gedanken experiment if you
will. Not a true Gedanken Schrodinger’s Cat type experiment, but answer
the following questions in your mind.

1)
What is the best NSAID for analgesia?
2)
Do oral or parenteral NSAIDs provide better pain relief?
Got your answers?
Good.
Based on the
conversations among staff, residents and nurses in the ED, oral or parenteral ketorolac
(AKA: IM Toradol) is the strongest/bestest/most fantastic/awesome NSAID out
there.
WRONG!
I know that regardless
of what I say from here on, some of you will stand by IM Toradol like a dying
loved one. That’s okay, I understand. It’s not your fault that you’ve
been brainwashed into thinking this way. Or maybe it’s anecdotal
experience from years of practice, and I’m just a young pup who doesn’t know
anything.
Just
hear me out.
What
is the best NSAID for analgesia?
There
isn’t one.
They’re all the same
when dosed appropriately. I cannot say it better than Grant Innes did in this 2005 review of ED pain medications.
“Although some
agents have been advocated for specific indications (eg, indomethacin for
gout), there is no compelling evidence
that any one NSAID is superior to any other—for any indication.
Consequently, NSAIDS should be selected based on convenience, cost, and
availability rather than on theoretical efficacy advantages.”
Important to note are
the dosing regimes for each NSAID, as they are more than often used in the ED:
Ibuprofen up to 800
mg QID
Naproxen up to 500 mg
TID
Ketorolac up to 10 mg
QID
Indomethacin up to 50
mg QID
*Edit: There is an important concept of ceiling effect with NSAIDs. I left this out here, and it is very important so we'll discuss it in part two of the NSAID saga. Thanks to reader @ETtube for pointing this out.
*Edit: There is an important concept of ceiling effect with NSAIDs. I left this out here, and it is very important so we'll discuss it in part two of the NSAID saga. Thanks to reader @ETtube for pointing this out.
Other NSAID regimes
are also found in this paper, but these are the most common ones in North
America.
But
what about IM toradol? It always works for my patients.
I don't know but
maybe these these guys know the
answer.


That's right, Sanjay Arora and Mel Herbert from EM:RAP
actually wrote a paper on this. 6 years ago!
I highly suggest you
take 10 minutes of your day to read this great article in CJEM in 2007. The full text version is free as well.
Alternatively, I'll
summarize it here.
1994 Wright et al.– Retrospective
analysis of data that was collected by prior prospective survey.
800 mg ibuprofen po
vs. 60 mg ketorolac IM - NO DIFFERENCE
in pain as rated by visual analogue scale (VAS)
1995 Turturro et al. – Prospective
DBRCT (Double blind randomized controlled trial).
800 mg ibuprofen vs.
60 mg ketorolac IM - NO DIFFERENCE
1998 Neighbor and Puntillo – Prospective DBRCT. 800 mg
ibuprofen vs. 60 mg ketorolac IM. All patients had self-assessed
pain between 5-8/10 on VAS.
NO
DIFFERENCE
*Funny
thing about this study is the author’s name is spelled as Neighbour with a “U”
in the text, but not in the references. Funny because the Canadian CJEM
autocorrect probably added the “U”. Maybe funny just to me.*
They also cite two
more trials comparing post-op pain with the same ibuprofen vs. ketorolac
dosing, but at this point, you get the picture.
Finally, all of these
studies compared 60 mg of ketorolac
IM to 800 mg of ibuprofen. Who
actually gives 60 mg? I've never seen it where I work, where 30 mg is
the standard dose. So, maybe ibuprofen is actually better than the 30 mg
of IM ketorolac that we give.
Some
of you may say, “I use the toradol for the placebo effect of an
injection. You can’t argue with that.”
Sorry,
someone studied that too.
This study by Schwartz et
al. was a prospective DBRCT in
which patients “were unknowingly given
800 mg oral ibuprofen in a flavoured drink and then given either a placebo IM
injection or a placebo pill.” No patient really received any IM
medication in either group, and there was similarly no difference in the VAS
between the two groups. So IM for
placebo effect only also appears unwarranted.
Also,
that study design is kick ass!
Treatment
bottom line:
There
is no difference between NSAIDs when it comes to pain control. Just use
an adequate dose of whichever you choose.
IM
ketorolac still has a role in vomiting patients or those unable to take po
meds, but don’t kid yourself that it’s a “stronger” medication. It’s not.
Despite all of
this, I agree that some NSAIDs work better for certain people? Why is
this?
Watch for parts
2 and 3 of the NSAID discussion, where we'll talk about this and much
more.
*Personal disclosure:
I use ibuprofen almost exclusively, but also use Naproxen, as the BID (can go
TID) dosing regimen generally means patients will be more compliant and
hopefully have better pain control for a greater duration. When we
discuss side effect profiles in the coming weeks, you'll see why I don't use
ketorolac.
Cheers,
SOCMOBEM
References:
Innes
GD, Zed PJ, Emerg Med Clin North Am. 2005
May;23(2):433-65, ix-x.
Arora
S, Wagner JG, Herbert M. CJEM. 2007 Jan;9(1):30-2.
Schwartz
NA, et al. Acad Emerg Med. 2000 Aug;7(8):857-61.
Tuesday, 5 February 2013
Battle Preparation: Getting Ready for Your First Shift in the ER
Today is a first for the SOCMOB blog, as we have our
first guest blogger. Damon
Tedford is one of my fellow EM residents, and is also in his final year of
training. Combining his military
background with the works of Cliff Reid and Scott Weingart, Damon had the
fantastic idea of creating a checklist
to familiarize oneself with the ED prior to their first shift. This will be released in two parts, a walk-about checklist today,
followed by a list of key questions later in the week.
*For part 2, click here.
*For part 2, click here.
Battle Preparation: Getting Ready for Your First
Shift in the ER
As the end of residency approaches, I often hear of
the tumultuous emotional trajectory that awaits the recently certified ER doc.
"Plan for three months of fear. It slowly gets easier after
that." I expect some growing pains after shedding the training
wheels, but have we not figured out a better way of assisting physicians with
this transition? After all, it is a yearly event.
In the few places I have interviewed, it would seem
that buddy shifts are the norm for newcomers. Physicians are eased into
their working environment over a number of shifts with a local, experienced
physician. It is a great, but imperfect idea, as the value of the orientation
depends on the cases of the day and what your mentor thinks you need to know.
In addition to these shifts, I plan on adding a more active and ordered
approach, leaving less to chance.
Before my medical days, I trained as an army officer
in the Canadian Forces, and if anyone can do order, it's the army.
During those days, we were taught a regimented approach to mission
planning. We called the process
"Battle Procedure." Reconnaissance, or a "Recce," is
a key component of Battle Procedure, so much so that all army leaders know the
axiom, “Time on recce is seldom wasted”.
During the planning stage, a commander will draft a recce
plan to identify factors that will waylay the mission (What equipment do I have
at my disposal? What aspects of the ground will impact my team? Where am I
vulnerable and how can I mitigate that risk?) These are some examples of
questions the leader seeks to answer during his recce. During the
recce, the leader walks the ground with a plan in mind. If this is impractical, he/she reviews
maps, satellite photography, or accounts from first-hand witnesses to get a
sense of the environment he/she will be operating. The commander then
completes a plan and shares it with the team. Together they may
"war-game" it, playing out each phase of the operation, identifying
oversights or unique aspects of the operational environment that necessitate
changes to how they have done business in the past.
Battle Procedure is a deliberate process, and one I
have used to work through some complex problems. If the military analogy
does not work for you, have a listen to Scott Weingart's Podcast #49 - Mind ofthe Resus Doc: Logistics over Strategy. It's one of my favorites and a
major inspiration for the checklists you will find below.
Here at SOCMOBEM, we have completed a recce plan for
the new ER physician, but this could easily be used by anyone new to the
department. Our goal is to ease the transition of new ER team members and
get them ready for peak performance on day one.
Identifying the key tasks we could be called upon to
complete during our first shift, we have created a list of equipment for time
sensitive resuscitation tasks as well as those that are more regular but
routine. Finding the equipment before your first shift prevents loss of
valuable time and also improves department flow. However, the document is
more than a medical scavenger-hunt.
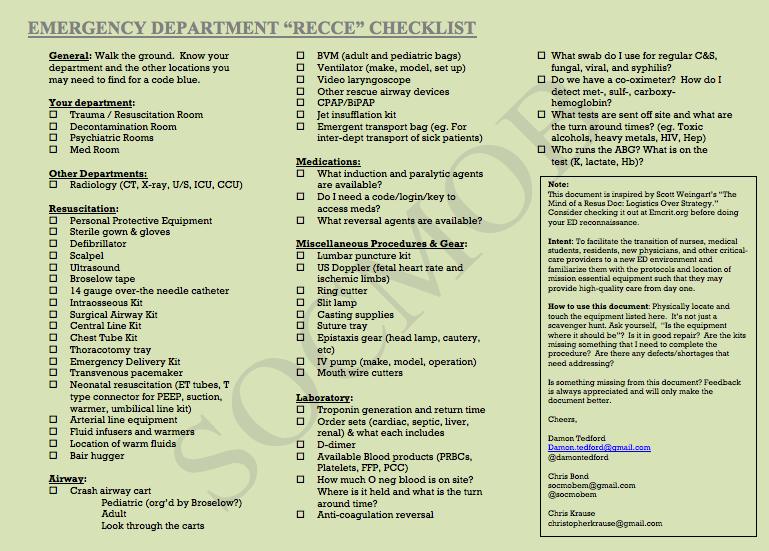
While
checking off items, ask yourself:
What is the state of repair of the equipment?
Are there shortages of essential items within the
procedure bundles that I will need to complete the task?
Would I be able to set up this ventilator alone?
How do I see a resuscitation playing out here?
Does equipment location make sense?
Where could things potentially go wrong for my team and
what could I do about it?
You get the idea.
With a fresh set of eyes, we may identify
opportunities to improve patient care and efficiency. A word of caution: no one likes a
know-it-all. Unless patient safety is an issue, save the
recommendations for an appropriate time and venue and deliver those suggestions
tactfully.
The second document will contain a list of questions
that will guide the conversation between mentor and new ER physician.
Perhaps it could be done over a coffee. Some examples of these
questions include:
What services are available after hours?
How do we handle mass casualties?
Do we have a massive transfusion protocol?
Where can I find this and other protocols?
We hope these posts help those who find themselves in
a new emergency department. If you have suggestions, let us know.
Peer review is key to improvement.
Cheers,
Damon
Thursday, 24 January 2013
New Surviving Sepsis Guidelines 2012: WTF?
Hey all, this is just a short snippet, not a full blog post. As the 2012 Surviving Sepsis Guidelines were just released, I'm just making a few comments and directing you to Scott Weingart's great podcast on the guidelines.
Everyone who takes care of emergent/critical care sepsis patients needs to take 18 minutes of their life and go listen to Scott Weingart's new Practical Evidence podcast on the 2012 Surviving Sepsis guidelines here.
The whole document is 60 some pages, but the big highlights for me are:
Good:
1)Lactate clearance now included as measure of tissue perfusion - But there is also some BAD with this one (see below).
2)Norepinephrine is 1st choice vasopressor for all patients.
3)Epinephrine as 2nd vasopressor, followed by vasopressin (new does 0.03 units/min)
4)Dopamine pretty much gone - Yay!
5)Protective lung ventilation strategies for sepsis induced ARDS
Bad:
1)Still recommending use of CVP goal of 8-12 mmHg to guide fluid therapy. Haven't we beaten this dead horse enough. See here
2)Still recommends SCvO2 to monitor tissue perfusion. This is fine if you have a CVL, but they do not make mention of lactate clearance being non-inferior to SCvO2. Also discussed in previous post on CVL (linked above).
3)Recommends delaying antibiotics up to 45 mins to give BCx. Uh, isn't time to antibiotics our #1 goal?
4)No recommendation for U/S of IVC, but still recommend static markers (HR/BP) to guide fluid responsiveness.
Scott does a great job of going over all of this and more in his podcast. A summary of the guidelines is also found there.
Cheers,
@SocmobEM
Everyone who takes care of emergent/critical care sepsis patients needs to take 18 minutes of their life and go listen to Scott Weingart's new Practical Evidence podcast on the 2012 Surviving Sepsis guidelines here.
The whole document is 60 some pages, but the big highlights for me are:
Good:
1)Lactate clearance now included as measure of tissue perfusion - But there is also some BAD with this one (see below).
2)Norepinephrine is 1st choice vasopressor for all patients.
3)Epinephrine as 2nd vasopressor, followed by vasopressin (new does 0.03 units/min)
4)Dopamine pretty much gone - Yay!
5)Protective lung ventilation strategies for sepsis induced ARDS
Bad:
1)Still recommending use of CVP goal of 8-12 mmHg to guide fluid therapy. Haven't we beaten this dead horse enough. See here
2)Still recommends SCvO2 to monitor tissue perfusion. This is fine if you have a CVL, but they do not make mention of lactate clearance being non-inferior to SCvO2. Also discussed in previous post on CVL (linked above).
3)Recommends delaying antibiotics up to 45 mins to give BCx. Uh, isn't time to antibiotics our #1 goal?
4)No recommendation for U/S of IVC, but still recommend static markers (HR/BP) to guide fluid responsiveness.
Scott does a great job of going over all of this and more in his podcast. A summary of the guidelines is also found there.
Cheers,
@SocmobEM
Subscribe to:
Posts (Atom)