Today is a first for the SOCMOB blog, as we have our
first guest blogger. Damon
Tedford is one of my fellow EM residents, and is also in his final year of
training. Combining his military
background with the works of Cliff Reid and Scott Weingart, Damon had the
fantastic idea of creating a checklist
to familiarize oneself with the ED prior to their first shift. This will be released in two parts, a walk-about checklist today,
followed by a list of key questions later in the week.
*For part 2, click here.
*For part 2, click here.
Battle Preparation: Getting Ready for Your First
Shift in the ER
As the end of residency approaches, I often hear of
the tumultuous emotional trajectory that awaits the recently certified ER doc.
"Plan for three months of fear. It slowly gets easier after
that." I expect some growing pains after shedding the training
wheels, but have we not figured out a better way of assisting physicians with
this transition? After all, it is a yearly event.
In the few places I have interviewed, it would seem
that buddy shifts are the norm for newcomers. Physicians are eased into
their working environment over a number of shifts with a local, experienced
physician. It is a great, but imperfect idea, as the value of the orientation
depends on the cases of the day and what your mentor thinks you need to know.
In addition to these shifts, I plan on adding a more active and ordered
approach, leaving less to chance.
Before my medical days, I trained as an army officer
in the Canadian Forces, and if anyone can do order, it's the army.
During those days, we were taught a regimented approach to mission
planning. We called the process
"Battle Procedure." Reconnaissance, or a "Recce," is
a key component of Battle Procedure, so much so that all army leaders know the
axiom, “Time on recce is seldom wasted”.
During the planning stage, a commander will draft a recce
plan to identify factors that will waylay the mission (What equipment do I have
at my disposal? What aspects of the ground will impact my team? Where am I
vulnerable and how can I mitigate that risk?) These are some examples of
questions the leader seeks to answer during his recce. During the
recce, the leader walks the ground with a plan in mind. If this is impractical, he/she reviews
maps, satellite photography, or accounts from first-hand witnesses to get a
sense of the environment he/she will be operating. The commander then
completes a plan and shares it with the team. Together they may
"war-game" it, playing out each phase of the operation, identifying
oversights or unique aspects of the operational environment that necessitate
changes to how they have done business in the past.
Battle Procedure is a deliberate process, and one I
have used to work through some complex problems. If the military analogy
does not work for you, have a listen to Scott Weingart's Podcast #49 - Mind ofthe Resus Doc: Logistics over Strategy. It's one of my favorites and a
major inspiration for the checklists you will find below.
Here at SOCMOBEM, we have completed a recce plan for
the new ER physician, but this could easily be used by anyone new to the
department. Our goal is to ease the transition of new ER team members and
get them ready for peak performance on day one.
Identifying the key tasks we could be called upon to
complete during our first shift, we have created a list of equipment for time
sensitive resuscitation tasks as well as those that are more regular but
routine. Finding the equipment before your first shift prevents loss of
valuable time and also improves department flow. However, the document is
more than a medical scavenger-hunt.
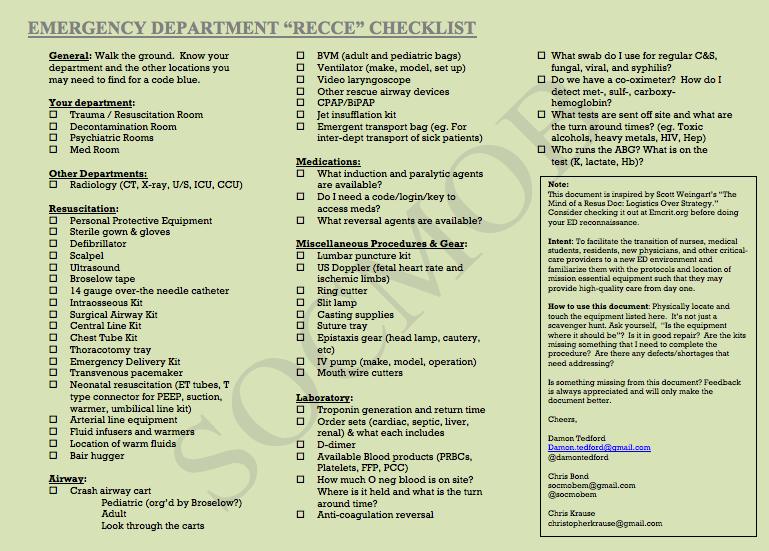
While
checking off items, ask yourself:
What is the state of repair of the equipment?
Are there shortages of essential items within the
procedure bundles that I will need to complete the task?
Would I be able to set up this ventilator alone?
How do I see a resuscitation playing out here?
Does equipment location make sense?
Where could things potentially go wrong for my team and
what could I do about it?
You get the idea.
With a fresh set of eyes, we may identify
opportunities to improve patient care and efficiency. A word of caution: no one likes a
know-it-all. Unless patient safety is an issue, save the
recommendations for an appropriate time and venue and deliver those suggestions
tactfully.
The second document will contain a list of questions
that will guide the conversation between mentor and new ER physician.
Perhaps it could be done over a coffee. Some examples of these
questions include:
What services are available after hours?
How do we handle mass casualties?
Do we have a massive transfusion protocol?
Where can I find this and other protocols?
We hope these posts help those who find themselves in
a new emergency department. If you have suggestions, let us know.
Peer review is key to improvement.
Cheers,
Damon
Great stuff Damon! Interesting that when I worked as a ED Tech, we had a similar checklist that we had to know so we could get the stuff for the Doc's. When you're the one in charge, you better know the details as well.
ReplyDeleteThanks for you comment. No one wants to be flailing for equipment when seconds count. Best to plan ahead.
ReplyDelete